
Two new studies demonstrate a link between Medicaid expansion and positive health outcomes, adding quantitative evidence to inform the nation’s ongoing debate about health insurance coverage.
Medicaid is a health insurance program for people who don’t have sufficient income or resources to otherwise attain health insurance. It is funded by both state and federal governments, but is managed at the state level. As of March 2019, 65,949,108 individuals were enrolled in Medicaid, and 6,662,765 were enrolled in the related Children’s Health Insurance Program (CHIP), according to the Centers for Medicare and Medicaid Services.
In 2014, an expansion of Medicaid eligibility to US citizens and permanent residents who earned up to 138% of the federal poverty level took effect as a provision of the Patient Protection and Affordable Care Act (ACA), which was signed into law by President Barack Obama in 2010.
The main group affected by this change was low-income childless adults. Before the ACA, the criteria for Medicaid eligibility generally required that adults either had to be disabled, at or below the federal poverty level with children between the ages of 6 and 19, or at or below 133% of the poverty level for pregnant women or families with children under the age of 6.
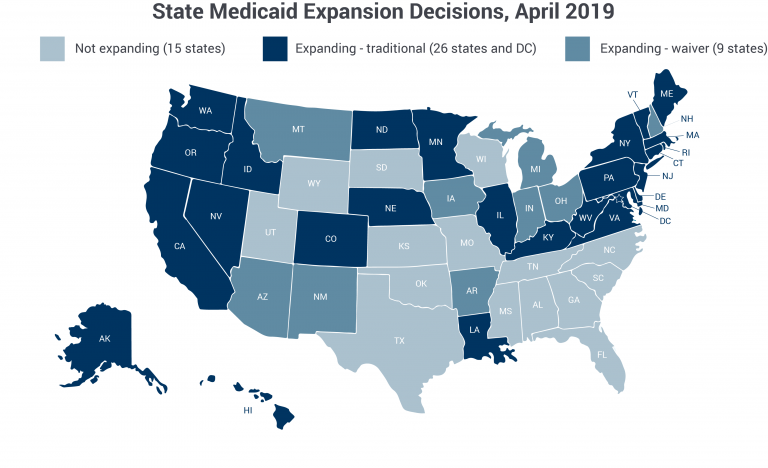
However, not all states have adopted the expansion. A 2012 Supreme Court ruling held that states could effectively opt out of Medicaid expansion without jeopardizing their existing federal funding for the program. As of April 2019, 35 states and the District of Columbia had implemented the expansion. States that opted out of the expansion continue to set their own eligibility requirements, leaving many low-income adults without an affordable option for health insurance.
This provided researchers with a kind of natural experiment: they could exploit the fact that some states opted to expand Medicaid coverage while others did not and analyze whether differences in outcomes arose along these same lines.
It’s worth noting that while this situation enabled an observational comparison of states that did and did not expand Medicaid, an observational experiment is not the same as a randomized, controlled experiment. In other words, it cannot be used to establish causation. It can and did, however, reveal important associations.
Roughly 2,000 fewer cardiovascular-related deaths per year
A new study in JAMA Cardiology looks at the difference in death rates attributed to cardiovascular causes, including heart attack, heart failure, arrhythmia-related death, stroke, and diseases of the aorta and blood vessels. The key finding: middle-aged people who live in states that expanded Medicaid under the ACA are less likely to die of heart disease.
Sameed Khatana and his co-authors find that counties in Medicaid expansion states had, on average, 4.3 fewer deaths per 100,000 residents per year than counties in states that did not expand Medicaid. Put another way, mortality rates among residents in non-expansion states increased over the six years studied – from 2010 to 2016 – while mortality rates among residents in expansion states stayed flat.
Prior to the ACA expansion, deaths from cardiovascular causes were rising in parallel across the country explains Khatana, a fellow in cardiovascular medicine at the University of Pennsylvania. The rise, he says “is a trend that has only recently been recognized, and it’s not clear why cardiovascular mortality has stagnated or started to go up in the United States.” However, he adds, the nation’s high rates of diabetes and obesity could help explain the trend, though the area needs further research.
In further analysis of the data, the researchers found that counties with more low-income residents had a stronger association between Medicaid expansion and cardiovascular mortality, which, Khatana says, “fits in with what you’d imagine Medicaid expansion would do.”
However, he notes, “The Affordable Care Act is a complex piece of legislation, which impacted the healthcare system quite broadly.” He adds that institutions that provide health care to low-income individuals, such as safety net hospitals (medical centers that provide health care to all, regardless of insurance status) and community health centers, have enjoyed improved financial health since the expansion went into effect. It is plausible, he says, that as the financial status of these institutions improved, quality of care improved too, and all patients receiving treatment there – regardless of insurance status – benefited.
Though the county-level effect might seem small, when multiplied to scale up to the number of middle-aged adults in states that expanded Medicaid, it translates to a difference of roughly 2,000 fewer deaths per year.
“Research like ours,” Khatana says, “is very important to quantitatively look at these policies that are being implemented.” He adds, “I think this line of questioning is useful not only to researchers but also to policy makers, patients, and just individuals.”
Medicaid expansion and racial disparities in cancer treatment
Blythe Adamson echoes a similar sentiment about her own work.
Her new research, which she presented at the 2019 American Society of Clinical Oncology Annual Meeting, and which is under review for publication, looks at the impact of Medicaid expansion on racial disparities in cancer treatment.
“This is one of the first times that we’ve seen such recent data be able to be used for real-time policy evaluation,” says Adamson, a health economist and Senior Quantitative Scientist at Flatiron Health, a technology and services company focused on cancer care.
Adamson and her co-authors looked at “timely treatment” – that is, initiation of cancer treatment within a month of diagnosis. Treatments included any systemic therapy, such as oral or intravenous chemotherapy or immunotherapy. Targeted treatments, such as surgery and radiation, were not included.
Adamson explains that the researchers designed the study to select for cases where patients should receive a systemic therapy in fairly short order because of the nature of the disease and the stage at which it was diagnosed.
For the purposes of this study, that meant patients diagnosed with advanced or metastatic forms of eight cancer types (non-small-cell lung, breast, urothelial, gastric, colorectal, renal cell, prostate cancer and melanoma). Patients were between the ages of 18 and 64. The sample included 34,067 patients diagnosed between January 1, 2011 and December 31, 2018.
The researchers were interested in timely treatment because it can be measured over a short period of time and because it’s more likely to be affected by policy changes than broader measures like overall survival might; without insurance, patients may be forced to forego treatment because of the cost.
“Having cancer treatment matters, because this is one of the most fragile, anxiety-filled moments in a patient’s journey,” Adamson says. “They just found out this terrible news, and to have this uncertainty — who’s going to pay for the treatment? Are they going to have coverage?”
What they found is that before Medicaid expansion, black patients were 4.9 percentage points less likely to receive timely treatment than white patients. After Medicaid expansion, black and white patients both saw increases in timely treatment. Black patients, though, saw a larger benefit. After states expanded Medicaid, racial disparities in timely treatment disappeared.
The researchers did not look at the implications timely treatment had on survival outcomes, though Adamson says that is a topic of interest for future research.
“Racial disparities exist across the care continuum, from screening, to diagnosis, to timely treatment,” she says. “Those disparities really accumulate and result in differences in health outcomes.” Her findings, however, provide some hope, she notes: “This is an intervention with evidence of effectiveness at improving racial equity.”
For more about Medicaid, see these tips for covering health care policy from POLITICO’s Joanne Kenen or read about a study showing that more minorities visited the doctor after Medicaid reform in Oregon.
Adamson, Blythe; et al. "Affordable Care Act (ACA) Medicaid Expansion Impact on Racial D